
Following a scan I uploaded last week of subaortic stenosis in a boxer, a veterinarian colleague of mine asked me a good question: how did I know I wasn’t catching mitral regurgitation?
Aortic stenosis (AS) and mitral regurgitation (MR) are both systolic, both travel away from the transducer, and arise from valves which are in continuity with one another. Temporarily and spatially, therefore, mitral regurgitant jets and aortic outflow traces are very close, and at times (if the MR is very eccentric and directed along the anteroseptal wall of the left atrium), virtually inseparable, with modified views needed to obtain separate traces for the two.
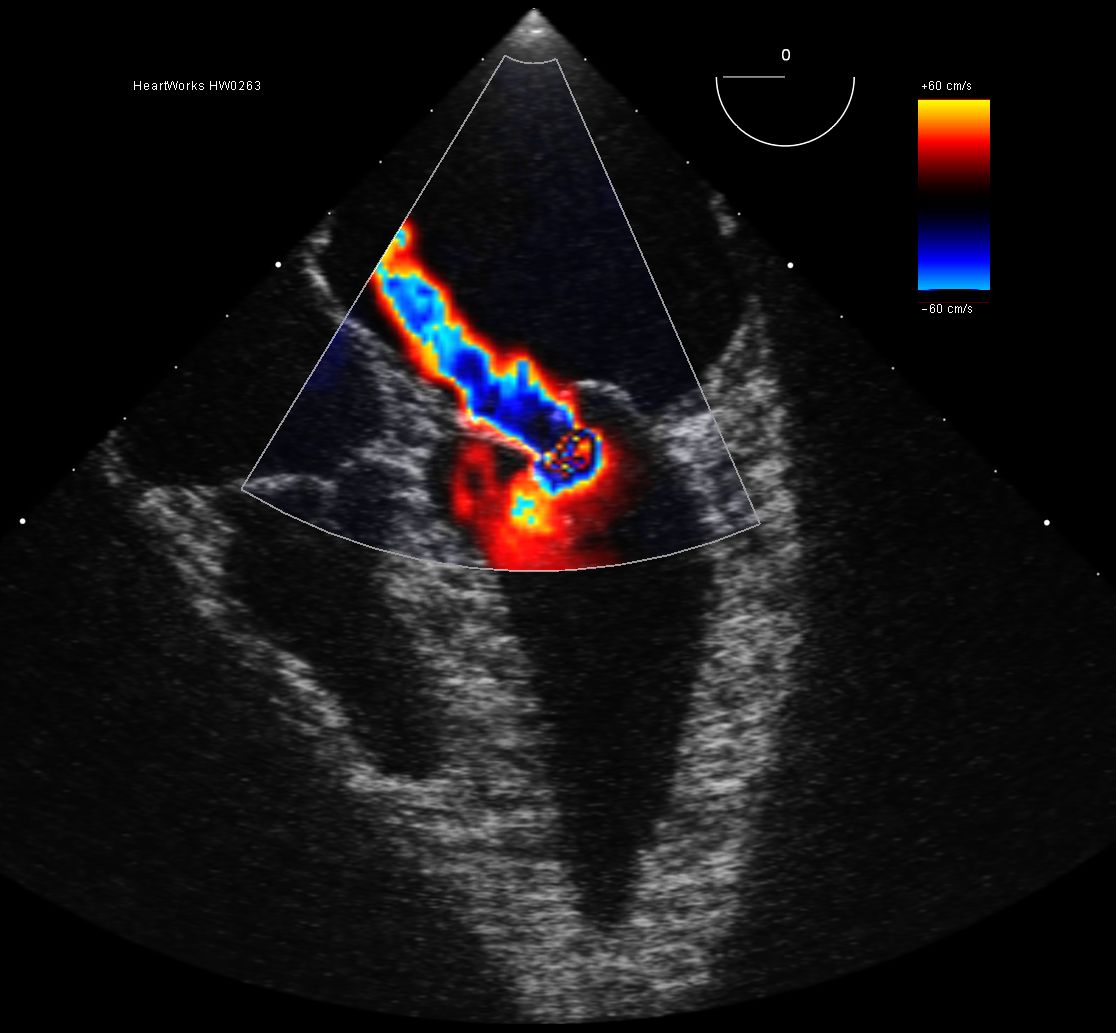
Significant MR is therefore a legitimate differential diagnosis in this case. Accidentally catching mitral regurgitation when intending to take an aortic outflow trace is entirely possible. I’ve created a scenario, shown above, in the HeartWorks transoesophageal (TOE) software package. This eccentric MR jet’s proximity to the left ventricular outflow tract (LVOT) and aortic valve is clearly illustrated. The LVOT is not fully opened up in the above view, but a slight upward tilt on transthoracic echo (TTE) or a slight rotation on TOE modifies this view to a ‘five chamber’ view:
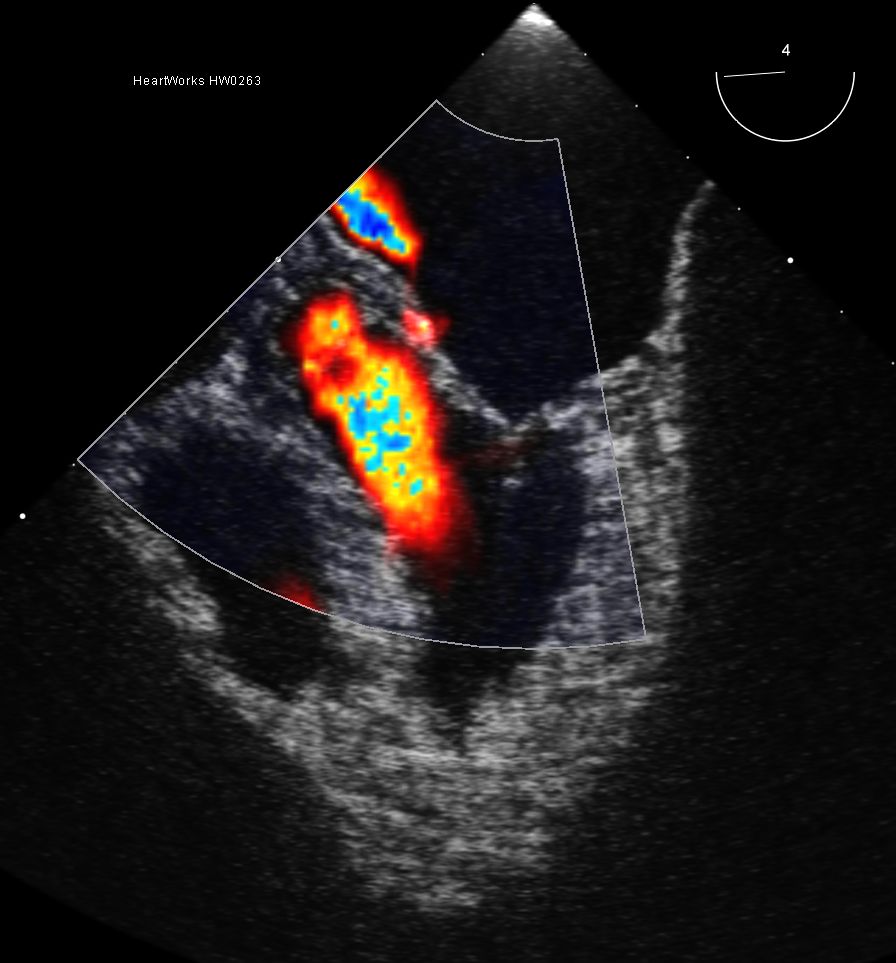
The MR jet remains partly visible, and in my experience, this would be far more obvious in real patients – it would be unusual to obtain this view and lose even the proximal isovelocity surface area (PISA) of the MR.
So, how can you be sure that you’ve really got the aortic outflow (in the presence of some degree of MR)?
1. Look for the closing click of the aortic valve. The closing click can be seen after each waveform in the continuous wave trace below:

2. Compare your MR and aortic outflow traces. MR will invariably have a smoother, more parabolic profile, and except in cases of significant left ventricular systolic impairment, will reach velocities of around 6m/s. If your “MR trace” is complete and reaching 3m/s in the presence of good left ventricular systolic function, it’s not an MR trace.
3. Compare your MR and aortic outflow traces side by side and check (or measure) your timings. MR will last longer than aortic outflow, beginning the moment the mitral valve closes (before ejection occurs from the aortic valve), and lasting until left ventricular pressure falls sufficiently for mitral valve opening. In other words, MR is pansystolic, beginning before and ending after aortic outflow – which is ejection systolic only. An ECG trace will help with timings, and many would consider a three-lead ECG a compulsory component of a full echocardiogram.
It may sometimes be possible to capture both traces on the same scale (often inadvertently). Here, you will see the aortic outflow trace superimposed on top of the MR, and the differences between the two are even more clearly discernible.