
Many veterinarians and mobile scanners own their own portable ultrasound machines. This equipment is coming into its own right now in the world of human scanning, as doctors re-purpose handheld and laptop-based ultrasound to check patients with suspected Covid-19. Portable ultrasound machines are so useful because they can be easily brought to patients’ bedsides – avoiding the risks of moving infected patients around hospitals – and are small enough to be cleaned thoroughly and efficiently, in a way that would be very difficult with trolley-based systems.
Veterinarians also use their ultrasound equipment to check the lungs of their patients, often when performing ‘FAST’ scans to rule out collapsed lung (pneumothorax).
In the following interest-only article we discuss the basics of lung ultrasound, and how any portable ultrasound scanner with a convex or microconvex probe can be adapted to lung scanning.
In normal patients, ultrasound cannot pass freely through the lungs because the alveoli are filled with air. This means that all we will see in normal patients are the pleural line and A-lines. We will not see fluid, lung tissue or B-lines in normal patients.
What are A-lines?
In normal patients (as well as in other conditions like asthma and COPD in humans and animals – but not COVID19), the bright white echogenic pleural line will be reverberated down the screen. This is termed an ultrasound artefact (the A-lines are not ‘real’). Each A line is equidistant from the next.
Lung sliding
Another normal finding is lung ‘sliding,’ which can be seen with regular breathing. This is simply the parietal pleura sliding against the visceral pleura (see video below).
In diseased lung, sliding is frequently absent, and A-lines are obscured by B-lines.
What are B-lines?
In patients with interstitial pneumonia and diffuse alveolar damage, B-lines will be seen. There are vertical lines which arise from the pleural line, and extend all the way down the screen, obscuring A-lines. Their number increases with decreasing air content. At least 3 B-lines must be seen between a single rib space for a positive diagnosis.

With pulmonary oedema, B-lines are seen universally, but in some diseases, distribution can be patchy. It is important, therefore, to check the patient from multiple views.
Irregular pleural lines
Thickened and irregular pleural lines may also be accompanied by lack of sliding. There may also be hypoechoic (dark) regions within the pleura.
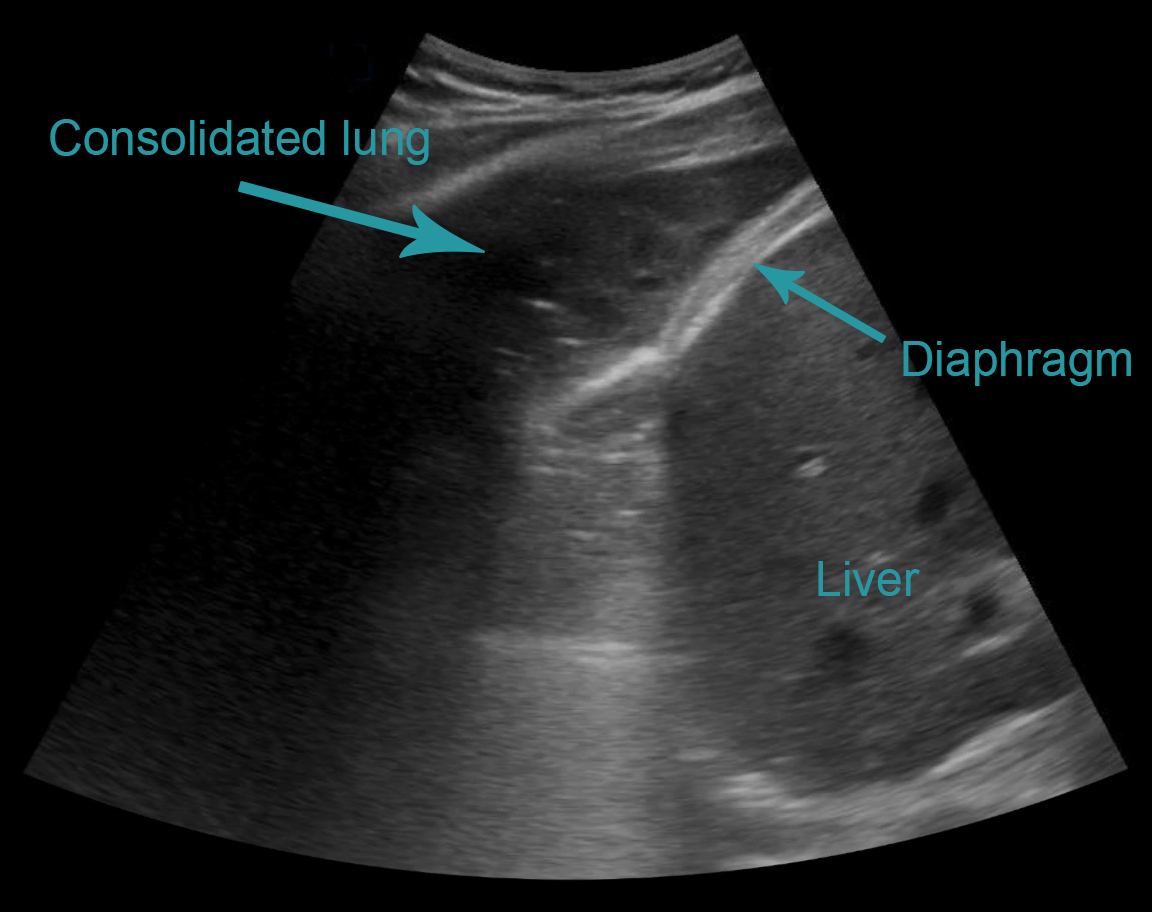
Consolidated lung
Also referred to as ‘lung hepatisation,’ because the lung appears similar to the liver. The alveoli become filled with fluid, allowing the ultrasound energy to pass through without excessive scattering and loss, and return to the probe and create an image.
The most common findings so far reported in Covid-19 patients are:
B-lines
Consolidated lung
An irregular pleural line