When I first began seriously scanning feline hearts (ten years ago now), I would occasionally come across patients with aliasing colour Doppler flow in the right ventricular outflow tract and mildly elevated velocities in the outflow tract and through their pulmonary valve. This was an isolated, somewhat baffling finding, because:
While I was new to scanning cat hearts, I thankfully wasn’t new to echocardiography. I’d already been through my baptism of fire that is being a novice with echo; hence, when I saw this in cats, I would mention it as a minor finding only, if I was sure it was clinically insignificant.
For people with less experience, however – perhaps learning to scan cats whilst still learning to ‘master’ echo (if one ever can!) – seeing unexpected turbulence like this can be extremely worrying. I remember the novice and improver stages very well; being hyper-alert for any abnormality, and as worried about missing something as you are excited about the prospect of finding something interesting. Seeing something like this without a lot of prior experience would undoubtedly have sucked hours of my time in an evening, poring over journal articles, going off on wild tangents, and probably calling the patient back for a rescan after learning about all sorts of obscure measurements and ratios I could have taken!
I cannot tell you exactly when I stopped really thinking about it at all, but there must have been a point at which I just incorporated it into my internal encyclopaedia: a benign explanation for a murmur in an otherwise normal cat.
In 2020, Farasin et al. recruited 61 cats with heart murmurs noted during auscultation and an echo report which noted dynamic right ventricular outflow tract obstruction. In their simple but ingenious study design, they varied the pressure of the probe against the chest wall, and demonstrated that dynamic right ventricular outflow tract obstruction (DRVOTO) could be lessened and worsened by a change of probe pressure. They therefore demonstrated the iatrogenic nature of this phenomenon in apparently healthy cats. The same effect can be caused with a stethoscope during auscultation, which would often be the reason for the echo referral in the first place.
To be clear, DRVOTO cannot automatically be dismissed as insignificant. Only after performing a full, through echocardiographic examination and finding no other signs of cardiac abnormalities, including no structural cause of the DRVOTO itself (i.e. no right ventricular hypertrophy or congenital abnormality), can DRVOTO be deemed to be benign/iatrogenic.
DRVOTO does of course accompany many cardiac diseases, and in cats, the most common of these is in those exhibiting a hypertrophic cardiomyopathy phenotype. While we focus heavily on left ventricular wall thickness in this disease, the right ventricle is also frequently affected.
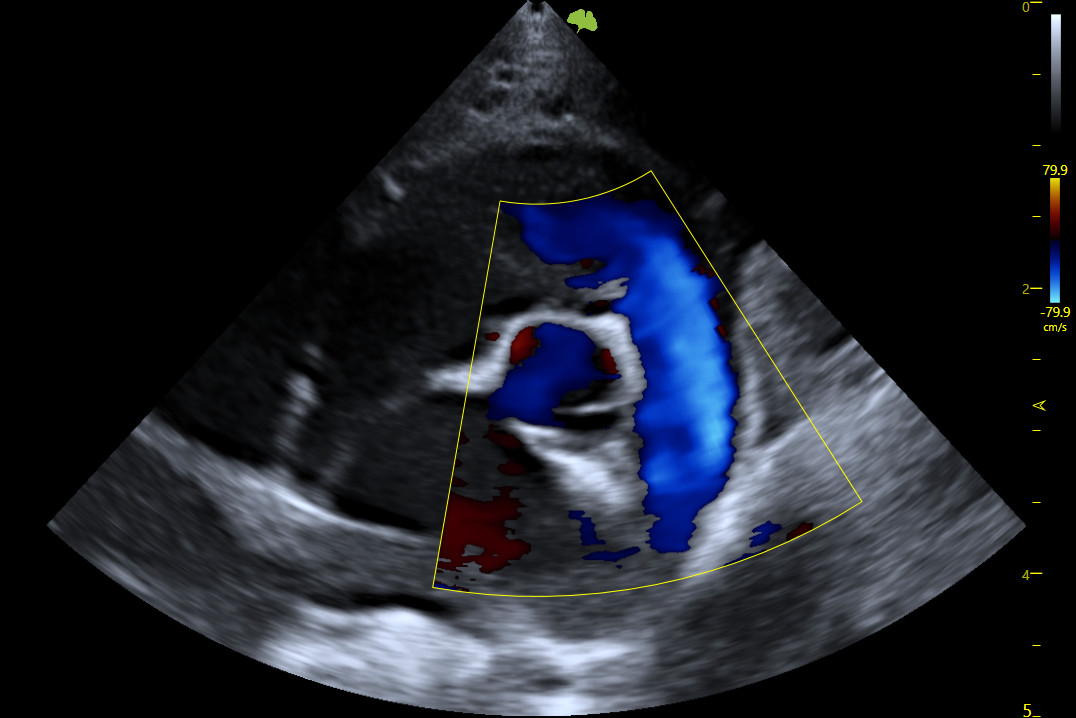
Below: Normal, laminar flow in the right ventricular outflow tract and pulmonary artery.
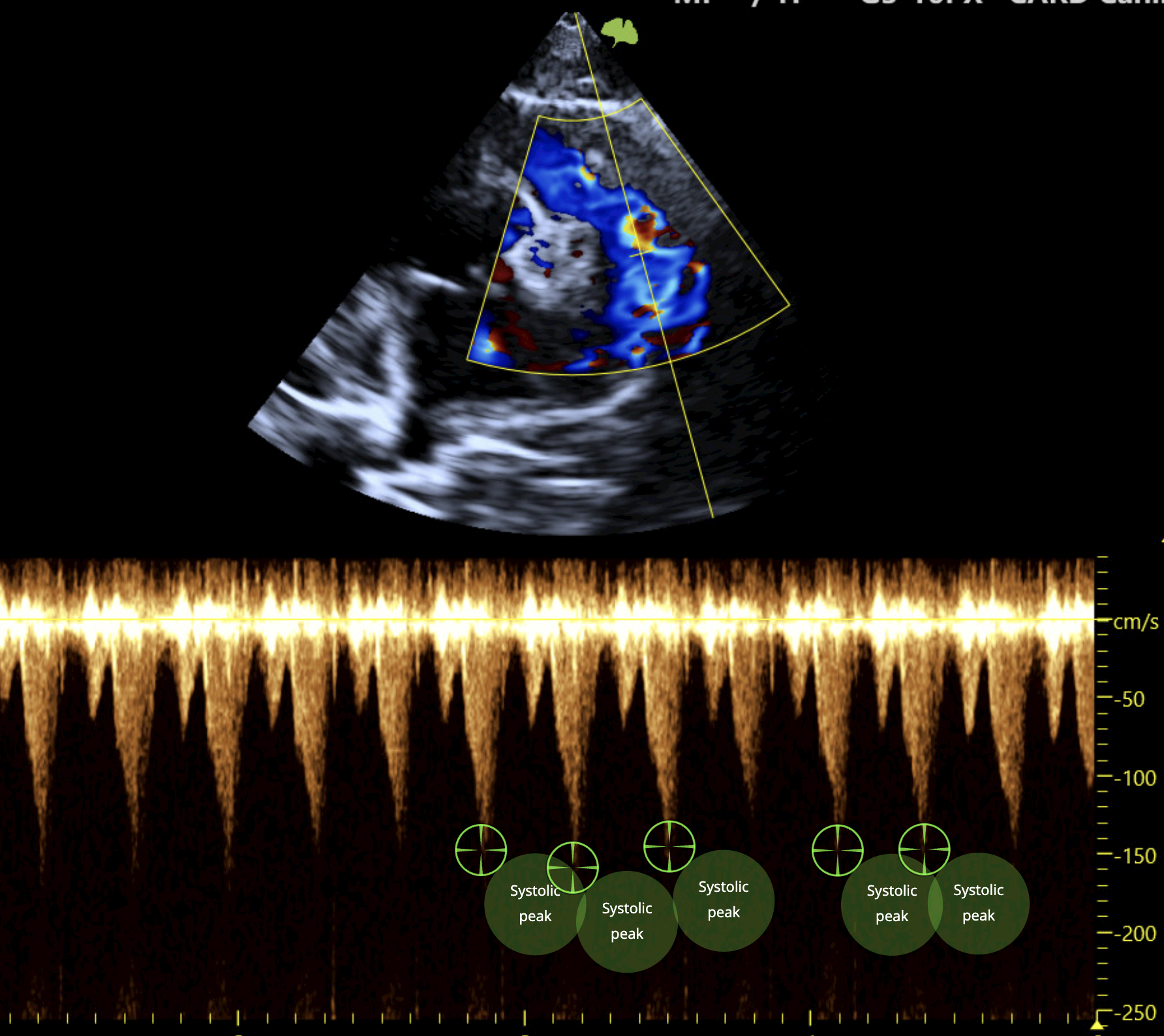
Below: Turbulent flow in the right ventricular outflow tract and pulmonary artery, with a late-peaking continuous wave Doppler trace, showing mild dynamic outflow tract obstruction. Systolic peaks have been measured by Quantum AI.
Next time you see turbulent, high-velocity flow in the right ventricular outflow tract, perform a careful inspection for any other cardiac abnormalities. If there are none, then possibilities are:
The turbulence you see is likely to be benign if your patient is otherwise healthy and there is no other explanation for the murmur that you hear.
References
Ferasin L, Ferasin H, Kilkenny E. Heart murmurs in apparently healthy cats caused by iatrogenic dynamic right ventricular outflow tract obstruction. J Vet Intern Med. 2020;34:1102–1107. 10.1111/jvim.15774