
Performing LV dimension and wall thickness measurements on dogs and cats should be straightforward, but unfortunately for us, it is anything but. The heterogeneity of measurement techniques, modalities (B-mode or M-mode), imaging planes (long- or short-axis) and species differences all combine into an absolutely mind-blowing mix.
Below, I will go into all of these differences, but for cats I will exclusively discuss B-mode measurements. M-mode really is a thing of the past and while I understand why some people continue to use it in dogs (if only to compare measurements with published normal values acquired using M-mode), it’s probably high time it was retired from feline echocardiography. Why make something that’s already hard, even harder?
If you’d like to be updated when another article and tutorial video like this comes out, please sign up to the newsletter here. If you’re an M-mode purest and want to send me hate mail (or, failing that, just your different opinion), you can do so here.
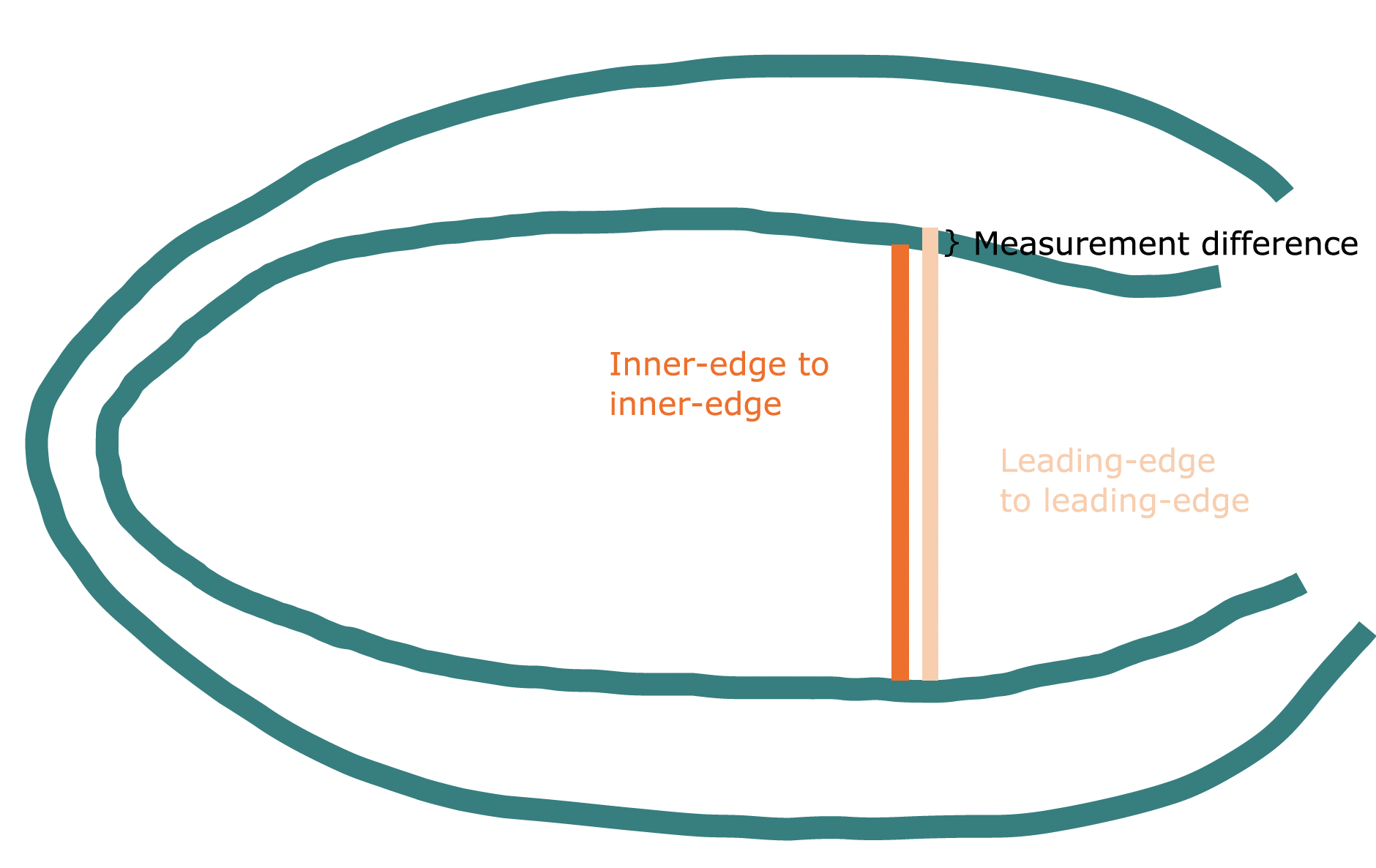
In dogs, M-mode measurement technique is leading-edge to leading-edge. This is because it M-mode measurements began in the 1950s, from a time when endocardial definition was poor. The ‘leading-edge’ – the first strong reflection from a structure – was the most clear and reproducible point to use for measurements, and for various reasons (having to rethink any normal values established using the old technique, and ensuring everyone transitions across to the new method), we’ve simply never changed it since.
With B-mode (the 2D imaging mode you are most familiar with), the measurement technique is inner-edge to inner-edge. This is because B-mode evolved when endocardial definition was much better, and inner-edge to inner-edge measurements should more accurately reflect the true anatomy. In theory, M-mode measurements of LV dimensions and wall thickness should be fractionally larger than those performed by B-mode (Rishniw et al., 2021).
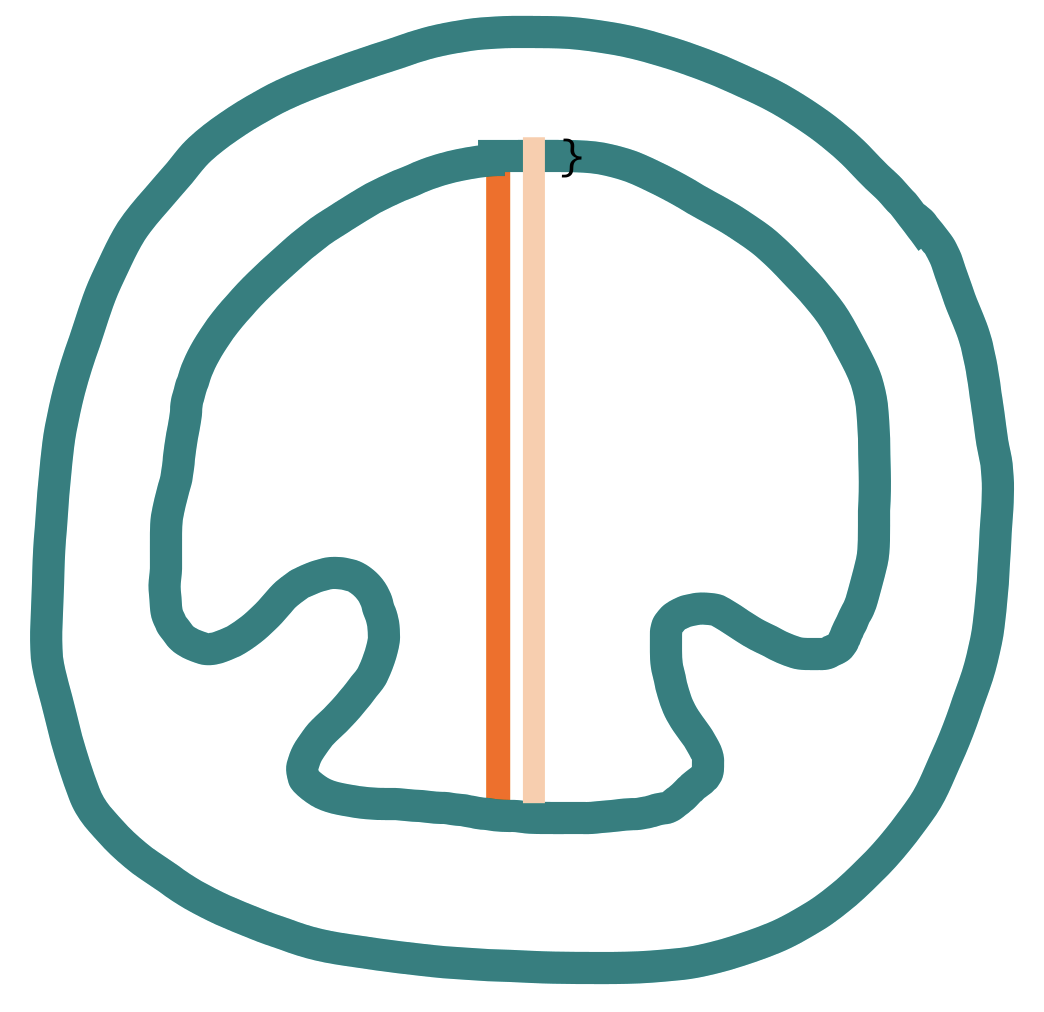
The diagrams below illustrates this point. While the measurement difference is small, it can be significant, and certainly in cats, M-mode and B-mode normal ranges are not interchangeable for this very reason.
Long-axis:
Short-axis:
What you need to remember:
If using B-mode, use inner-edge to inner-edge.
If using M-mode, use leading-edge to leading-edge.
There are no agreed cut offs for normal vs abnormal in dogs, nor any true consensus on how to normalise for body size. This was probably what you were looking for when you found this article, so I apologise for the disappointment. The good news, though, is that we do have a few very good studies that, more or less, agree with one another.
Some excellent work was performed by Cornell et al. in 2004, who retrospectively looked at 494 dogs of various breeds and calculated the exponents to normalise M-mode measurements in most dogs, with the caveat that extremes of body size might need separate consideration. They gave the formulae:
Indexed LVIDd = Measured LVIDd (cm) / Bodyweight (kg)
Indexed LVIDs = Measured LVIDs (cm) / Bodyweight (kg)
Indexed IVSd = Measured IVSd (cm) / Bodyweight (kg)
Indexed LVWd = Measured LVWd (cm) / Bodyweight (kg)
Once you perform this calculation, you can then refer to Cornell et al.’s published normalised values to check if your patient falls within the range of their published (admittedly rather wide) prediction intervals.
| Measurement | Mean indexed value | Lower 95% PI | Upper 95% PI |
|---|---|---|---|
| LVIDd (LV internal diameter, diastole) | 1.53 | 1.35 | 1.73 |
| LVIDs (LV internal diameter, systole) | 0.95 | 0.79 | 1.14 |
| IVSd (interventricular septum, diastole) | 0.41 | 0.33 | 0.52 |
| LVWd (LV free wall, diastole) | 0.64 | 0.33 | 0.53 |
While Cornell et al. only looked at M-mode measurements, Rishniw et al. surprisingly found that short-axis B-mode and M-mode measurements appear to be interchangeable in dogs, so work like the Cornell at al (2004) study remain relevant. If you are going to use Cornell as your go-to reference, just be wary of how wide the prediction intervals are and do not assume your patient is normal if they fall close to the upper 95% (or that they’re automatically abnormal just because they fall outside of it!).
Research published since the landmark Cornell paper have refined normal ranges further. In particular, in 2020 Esser et al split reference ranges into sighthounds and non-sighthounds, finding that bodyweight cannot be used to predict normal ranges in sighthound breeds.
In non-sighthounds, their formulae are:
| LVIDd (LV internal diameter in diastole) | 1.38 × BW0.322 |
| LVIDs (LV internal diameter in systole) | 0.87 × BW0.346 |
| IVSd (septum in diastole) | 0.36 × BW0.289 |
| LVWd (free wall in diastole) | 0.40 × BW0.261 |
These formulae give smaller mean normal values than the Cornell numbers, and narrower prediction intervals.
The ACVIM 2019 guidelines on the diagnosis and treatment of myxomatous mitral valve disease still reference the original Cornell et al. (2004) allometric scaling method for LVIDd, but provide a cut-off value of ≥1.7 normalised to bodyweight (lower than Cornell’s upper 95% prediction interval), which can be used along with other supporting evidence (left atrial size, symptoms) to stage dogs with MMVD and decide on treatment (Pimobendan). This normalised ≥1.7 value comes from the Boswood et al (2016) enrolment criteria for their ground-breaking Pimobendan trial, where the authors do not explain how they decided upon ≥1.7 specifically. However, the results of the trial were so powerful that it has simply stuck.
Cut-offs are provided below. Remember, this is only for dogs with myxomatous mitral valve disease. You cannot deem any and every dog with a normalised LVIDd ≥1.7 as abnormal – we simply do not have the evidence to know that this is true.
| Bodyweight (kg) | LVIDd (cm) |
| 1 | 1.7 |
| 2 | 2.1 |
| 3 | 2.4 |
| 4 | 2.6 |
| 5 | 2.7 |
| 6 | 2.9 |
| 7 | 3.0 |
| 8 | 3.1 |
| 9 | 3.2 |
| 10 | 3.3 |
| 11 | 3.4 |
| 12 | 3.5 |
| 13 | 3.6 |
| 14 | 3.7 |
| 15 | 3.8 |
| 16 | 3.8 |
| 17 | 3.9 |
| 18 | 4.0 |
| 19 | 4.0 |
| 20 | 4.1 |
The 2020 guidelines can feel confusing to read, but if you actually perform the measurements as suggested, it makes more sense. For 2D measurements, they recommend:
These should be taken from at least one long-axis view, and the short-axis view at papillary muscle level. Watch this 5 minute video to see what this actually means in practice:
Where focal hypertrophy is found, one should of course take additional measurements at this region of increased thickness. This is the most up-to-date measurement technique guidance we have for cats at time of writing (October 2025), but it might change in future guidelines.
There is significant inter-observer variability in wall thickness measurements in cats, even among board-certified expert echocardiographers. Unfortunately, this is highest for septal wall thickness measurements – the most frequently affected wall in cats with hypertrophic cardiomyopathy. There is some work going on at the moment on contrast-enhanced wall thickness measurements (where you inject a microbubble agent, such as SonoVue, flush it through with saline and use a contrast-specific preset or manually reduce your acoustic power so as not to pop the bubbles too quickly), and a theory that this will lead to greater reproducibility, but nothing has been published so far to verify this.
If you would like a handy wall chart of left atrial diameter, wall thickness and left ventricular internal diameter values for various body weights in cats, you can download it for free here.
The best way to improve measurement accuracy and reproducibility is to be part of a brainwashed cult.
The next best thing is to find a group of people who are serious about their echo and enjoy sharing their images and ideas. If you are looking for that, check out our programme, Confidence in Echocardiography. This comprehensive programme provides not only the training materials you need to become confident in your echocardiography, but also lifelong support in the form of webinars, video case walkthroughs, and a supportive community. If you have read this far in this article, we would definitely love to have you. If you would like to talk more about this, you can book a free Zoom call here.
If you are not quite ready to dive that deeply into echo, you can join our monthly small animal echocardiography newsletter to gain more exposure for free.
References
Cornell, C., Kittleson, M., Torre, P. et al. (2004). Allometric Scaling of M-Mode Cardiac Measurements in Normal Adult Dogs.
Esser, L., Bauer, A., Häggström, J., Wess, G. (2020). Left ventricular M-mode prediction intervals in 7651 dogs: Population-wide and selected breed-specific values.
Keene et al. (2019). ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs.
Luis Fuentes et al. (2020). ACVIM consensus statement guidelines for the classification, diagnosis, and management of cardiomyopathies in cats.
Rishniw, M., Corda, A., Spina, F. and Caivano, D. (2021). Two-dimensional echocardiographic measures of left ventricular dimensions agree with M-mode measurements in dogs.
Schober, K., Savino, S., Yildiz, V. (2017). Reference intervals and allometric scaling of two-dimensional echocardiographic measurements in 150 healthy cats.
Stowell, C. et al. (2024). Automated echocardiographic left ventricular dimension assessment in dogs using artificial intelligence: Development and validation.