
A kitten or puppy with a loud murmur always raises suspicion of a restrictive ventricular septal defect (VSD). ‘Restrictive’ sounds bad, but it’s actually the best case scenario for a VSD, because it means it is small.
A large defect will not be so restrictive to flow, and that’s a bad thing. It means a massive volume of blood will cross over from the left to the right ventricle, and pulmonary hypertension and congestive heart failure are very likely. A small, restrictive VSD can be tolerated for many years (or even for life), but will sound more dramatic on auscultation due to the much higher velocity shunt.
Thankfully, like little Ted whose images will be used to illustrate this article, most of the VSDs we come across are restrictive. The vast majority of them are also located in the left ventricular outflow tract (perimembranous VSDs).
If you are not used to seeing them, though, they’re not always easy to spot. Here are three views to spend a little extra time on with your colour Doppler when trying to demonstrate the presence (or absence) of the most common scenario: a restrictive, perimembranous VSD.
It is very difficult to see a small VSD on 2D imaging alone, but by placing your colour box over the outflow tract, aortic root and right ventricle, you stand a good chance of spotting the high-velocity left-to-right shunt on your very first few. In a young animal the shunt will almost always be left-to-right because blood is moving from the high pressure systemic ventricle, to the much lower pressure pulmonary system.
You can maximise your chances of seeing the shunt clearly by focusing your attention on the area you expect to see a VSD: reducing your depth, or zooming in over the outflow tract, aortic valve and aortic root are particularly useful.
Since blood is travelling through the defect towards your probe, it will be primarily coded in red, although you can expect a lot of turbulence and aliasing as well. Beginners can find it difficult to see a shunt, particularly at high heart rates, so freezing your image and then playing the clip in slow motion or moving through frame-by-frame is a good trick for noticing colour flow where it should not normally be.
Most perimembranous VSDs can be seen quite clearly from the basal short-axis view. You can describe the aorta like a clock-face when reporting where you can see the shunt most clearly. In the example below from an 8 week old French Bulldog puppy, it is at around 1 o’clock. Another common site is at around 10 o’clock.
Once you have your basal short-axis view on-axis (with the aorta circular in the middle), you can make minuscule movements with the probe head, pointing it slightly more towards the animal’s head to fan to aortic valve level, and then back towards you (wrist in towards the echo bed, probe head tilting very slightly towards yourself) to cut further into the left ventricular outflow tract. The aorta and outflow tract are just one long tube (with the aortic valve situated along it), so you need to be cutting through it at the same level as the defect in order to see the shunt.
If the VSD is there but you do not have it perfectly in plane, you should still be able to spot a lot of turbulence in the right ventricular outflow tract – the part wrapping around the aorta and leading out towards the pulmonary valve – which will give you a strong clue that you need to keep checking.
As before, optimising your depth or using zoom can help.
From either or both of these two views, you can of course further confirm the presence of a high-velocity shunt using your continuous wave Doppler. The better your alignment with the jet, the higher the velocity and cleaner the trace you will obtain. In a young animal, you should be obtaining velocities >4m/s through a restrictive VSD, so long as you are properly aligned with the jet.
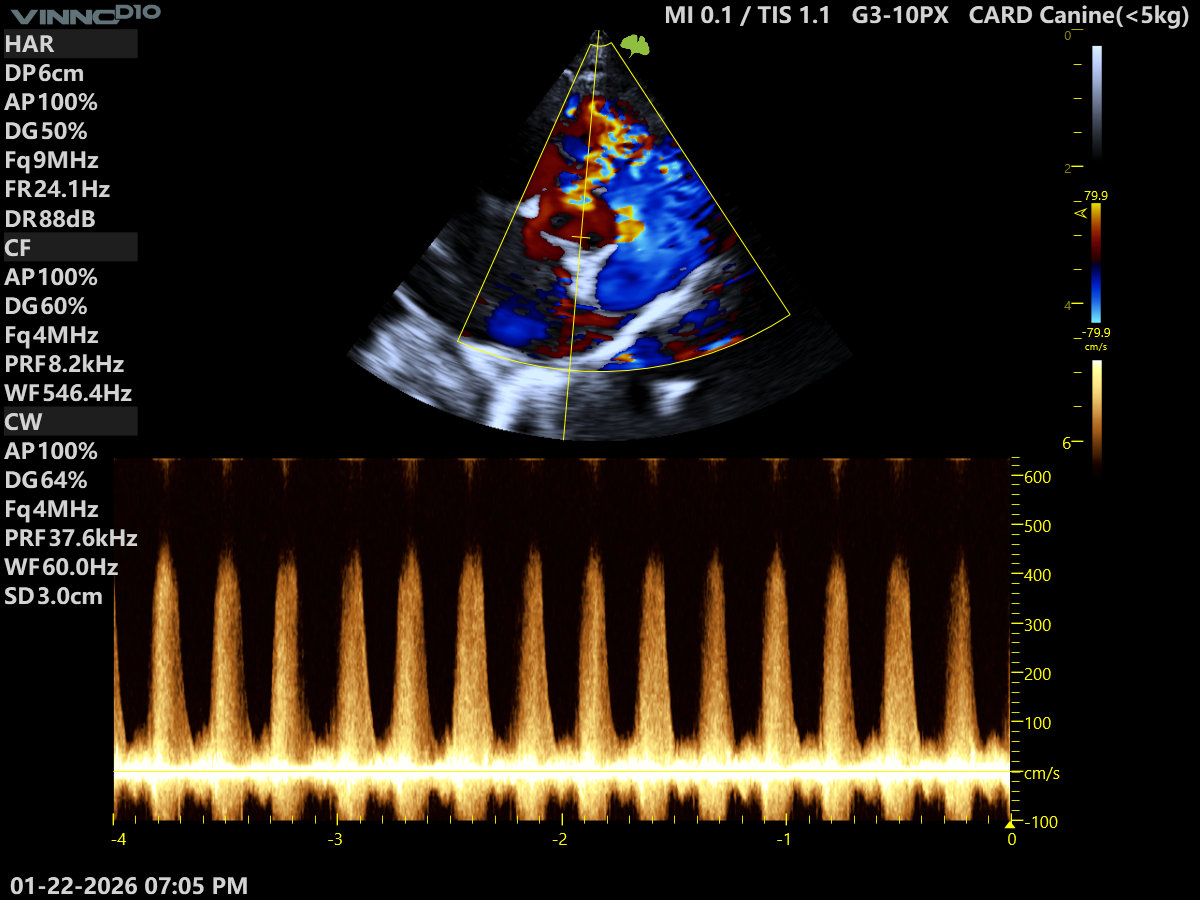
Why should the velocity be >4m/s?
Using a typical example, if LV systolic pressure is 125mmHg and RV systolic pressure is 25mmHg, the pressure gradient between the two chambers would be 100mmHg.
In this instance, using the simplified Bernoulli equation (ΔP=4v²) and rearranging for v:
v = √ΔP/4
v = √ 100/4
v = √25
v = 5
A pressure difference of 100mmHg between the left and right ventricle would mean that blood would shunt at a velocity of 5m/s. Long-standing disease can result in pressure equalisation between the two chambers and a reduced velocity, but this would be very unlikely in a puppy or kitten with a small VSD. In a young animal, a low velocity is more likely to mean that you are not properly aligned with the direction of flow (unless of course the VSD is very large).
You can rarely visualise a ventricular septal defect directly from the apical position, but you can see secondary signs of it. The most obvious one is a lot of turbulence in the right ventricle; colour flow will look very abnormal. This is a major clue that blood must be shunting into this chamber at high speed.
Another thing you can look out for is a mild, central jet of mitral regurgitation in what otherwise appears to be a normal mitral valve. Mild functional mitral regurgitation frequently accompanies VSDs due to the volume overload and dilatation of the left heart.
If you are not already subscribed, please do sign up to our free echocardiography newsletter. This is how we share interesting cases or teaching videos with you.
If you are serious about improving your confidence in echocardiography this year, then take action now and schedule a Zoom meeting with Catherine Stowell. This gives you an opportunity to discuss what stage you feel you are at with echocardiography right now, what your current challenges are, find out if you would be a good fit for our training programme.
We also have a fantastic online course called ‘Clinical decision-making with Echocardiography‘ from Professor Luis Fuentes, one of the world’s leading cardiologists. Her wonderful teaching style and wealth of experience brings echo alive, making it feel more relevant and exciting than ever before.
You can also check out one of our older videos on VSDs below: